Medicine is moving earlier.
Not only after the tumour grows. Not only after the scan changes. Not only after the heart fails, the pancreas collapses, or the patient reaches the specialist centre.
The next phase of personalised medicine is happening before the crash: immune staging, home monitoring, genomics platforms, safety prediction, price machinery and supply chains that decide whether care arrives early, late, or not at all.
The future is not waiting politely at the clinic door. The system is still built to react late.
| This is not another health news digest. It’s a twice-weekly readout of where evidence meets power and where power must turn into action. |
Diabetes care is moving before the crash

Diabetes has just given personalised medicine one of its clearest signals outside oncology.
The FDA expanded Sanofi’s Tzield for children aged 8 to 17 recently diagnosed with stage 3 type 1 diabetes. The goal is not cosmetic. It is to slow the loss of insulin production after diagnosis. This is medicine trying to protect function before more damage is locked in. But it is not a fairy tale either. Tzield carries serious safety warnings, including risks linked to infections. Earlier treatment still means harder choices, not easier ones. ( Reuters.)
At almost the same time, the FDA cleared Dexcom’s Stelo as the first over-the-counter continuous glucose monitor for children with diabetes who do not use insulin. That shifts monitoring closer to families, daily life and real behaviour, not just clinic appointments. ( Reuters.)
Put the two together and the direction is obvious. Personalised medicine is no longer only “find the mutation, give the drug.” It is becoming earlier, closer and more continuous: stage the disease, monitor the signal, protect function, and act before deterioration becomes normal.
That is exciting. It is also a policy headache.
Who gets access to early intervention? Who pays for monitoring? Who explains risk to families? Who decides when a child becomes “eligible enough”? And who makes sure this does not become another advantage for patients already close to the best systems?
The future of medicine is not only treating disease better. It is catching the crash before it happens.
IPM Latest
IPM joins Franco-Indian respiratory health meeting in Nice
IPM Alliance Executive Director, Denis Horgan, is in Nice tomorrow for “Respiratory Health: From Research to Daily Life,” a Franco-Indian scientific meeting focused on pollution, inflammation, nutrition, microbiota, AI, multi-omics and precision medicine in respiratory disease.
Held on 17 and 18 June 2026 with IHU RespirERA, Université Côte d’Azur and the Franco-Indian Campus, the event brings together French and Indian experts to build new research and innovation links. (Université Côte d’Azur / LIFE Graduate School)
For IPM, the message is clear: respiratory health is no longer only about treatment after disease appears. It is becoming a precision medicine challenge, where environment, data, early detection and system readiness must meet.
Public fights, private stakes
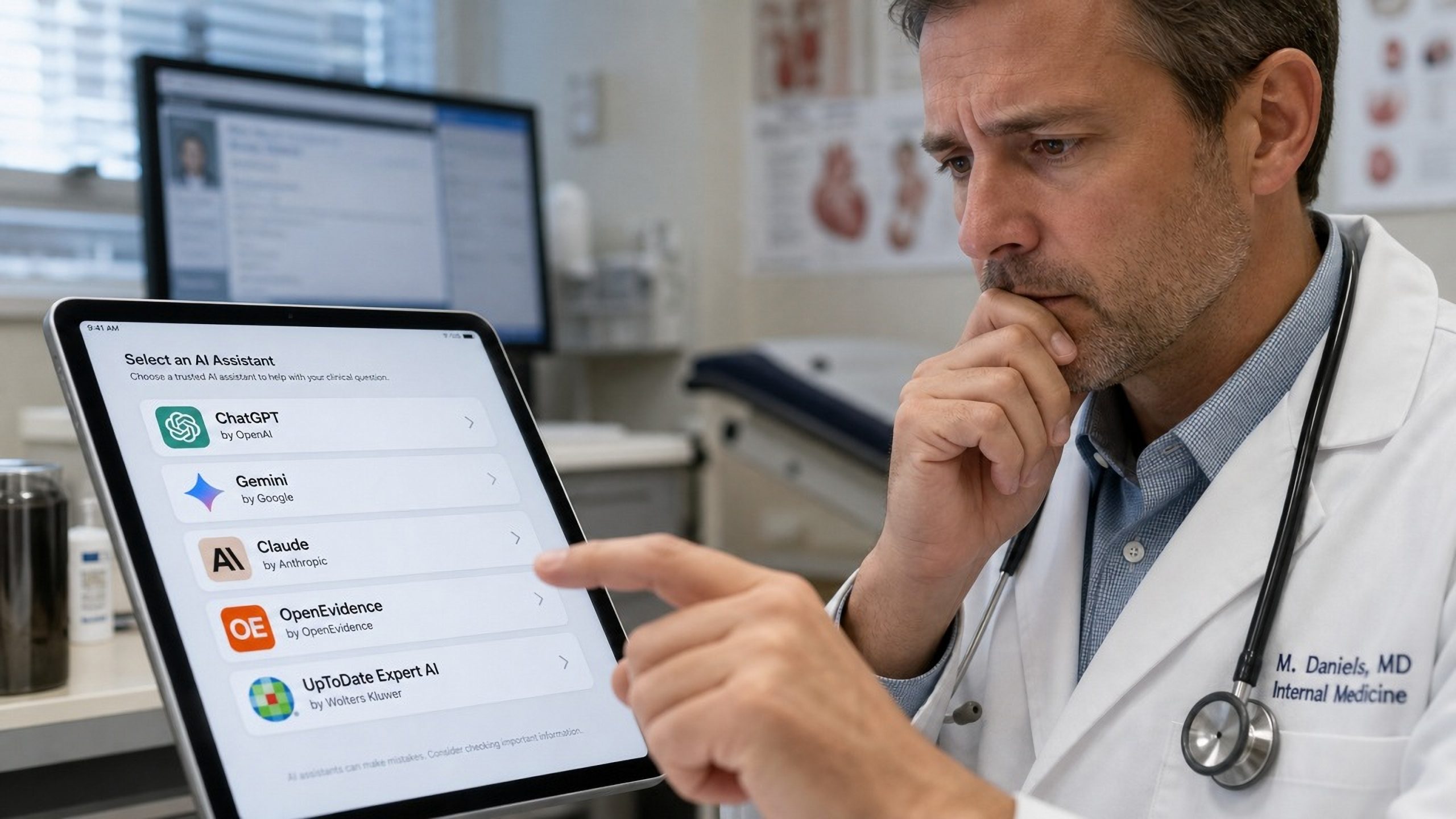
The AI doctor fight has started.
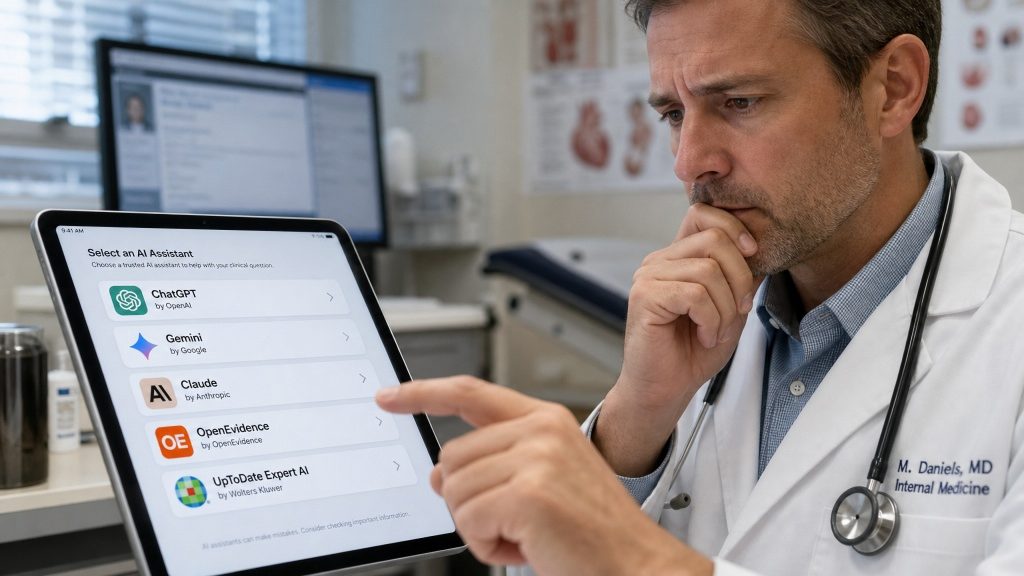
The public fight is about a paper. The private stakes are about trust at the bedside.
A Nature Medicine study landed like a grenade in the medical AI world. General-purpose models, including GPT-5.2, Gemini 3.1 Pro and Claude Opus 4.6, outperformed specialist clinical AI tools, including OpenEvidence and UpToDate Expert AI, across medical knowledge questions, clinician-alignment tasks and real clinical queries reviewed by blinded clinicians.
That is not a small headline. It questions the pitch behind a fast-growing sector: that clinical AI products are safer, smarter and more useful because they are built for medicine.
OpenEvidence did not sit quietly. In a public post on X, the company pushed back hard, welcoming rigorous evaluation but arguing that the study was flawed. Its critique pointed to issues such as benchmark contamination, scoring bias and the independence of the evaluation. In other words: the company’s message was not “AI should not be tested.” It was “this is not the test that should decide the story.” (OpenEvidence on X.)
The online reaction split fast. Some physicians saw the paper as proof that frontier models are catching or overtaking branded clinical tools. Others argued the benchmark may reward polished answers more than safe clinical judgment, source quality, recency or the ability to refuse when the question is unsafe. That matters. In medicine, a confident answer is not always a good answer.
For IPM, this is the real story. AI in medicine cannot enter care through branding, valuation or vibes. It needs independent evaluation, transparent methods, real-world workflow testing, citation quality, auditability and governance.
The winner is not the model with the loudest demo.
The winner is the one health systems can test, trust and control.
What breaks
No platinum, no pathway.
Precision oncology loves the future. Cancer care still runs on old drugs.
India raised price caps on cisplatin and carboplatin by 50% to tackle shortages of two essential platinum-based cancer drugs. These are not luxury medicines. They are workhorse treatments used across major cancers, and shortages have hit government hospitals particularly hard. (Reuters.)
This is the part nobody puts on glossy innovation slides.
A biomarker pathway means little if the basic chemotherapy is missing. A tumour board cannot solve an empty shelf. A precision oncology strategy still depends on procurement, raw materials, manufacturing economics and public hospitals that can keep essential medicines available.
This is not anti-innovation. It is the opposite. If health systems cannot protect the backbone, the breakthrough becomes a privilege.
Big tech wants the genome stack.
Samsung Electronics invested $175 million in Element Biosciences, becoming the U.S. genomics company’s largest shareholder. Element makes sequencing products, and Samsung has made clear where it wants this to go: genomics, multi-omics, AI, medical devices and digital health stitched together. (Reuters.)
This is not just another funding round.
It is a sign that personalised medicine is becoming a platform fight. The next gatekeeper may not be the company with the drug. It may be the company that controls the stack: sequencing, devices, data, AI, monitoring and the route from signal to decision.
Health systems need to ask the boring questions early: who owns the data, who validates the algorithm, who pays for the test, who integrates the result, and who is left out when the platform is not available?
The next access gap may be digital before it is clinical.
What breaks after approval
The drug works. Can the hospital handle it?
Some therapies do not fail because they lack impact. They fail because the system cannot safely deliver them widely enough.
Poolbeg Pharma is starting a UK trial of POLB 001, an oral drug being studied to prevent cytokine release syndrome in patients receiving teclistamab for blood cancer. The trial is small, early and investigational, with 30 patients across six NHS hospitals. So no hype. Not yet. (The Guardian; BioIndustry Association.)
Modern immunotherapies need more than approval. They need trained teams, monitoring, beds, escalation protocols, toxicity management and confidence outside a handful of specialist centres. If safety management improves, more patients may be able to receive complex therapies closer to where they live.
Approval opens the door.
Safety infrastructure decides how many patients walk through it.
Money and access
The price fight is becoming permanent machinery.
CMS has proposed a rule to establish a permanent framework for Medicare drug price negotiations from 2029. This is not another one-week pricing argument. It is the price fight becoming operating system. (Reuters.)
High-cost single-source drugs, combination regimens, small patient populations, companion diagnostics and long evidence timelines are all heading into a world where payers want predictable leverage. Companies want predictability too, but not at the price of losing pricing power.
Patients do not care which side wins the talking point. They care whether the drug is available, affordable and actually delivered.
The June watchlist
June is not done. The second half of the month brings decisions and meetings that could shape the next access fights.
| 19 June, EU & online: |
| European Commission HTA webinar for high-risk medical devices and IVD developers. |
| 22 June, UK: |
| The MHRA consultation on gene therapy regulation closes. (MHRA.) |
| 22-25 June, Amsterdam: |
| EMA committee for medicinal products for human use plenary. |
| 22-25 June, San Diego, US: |
| BIO International Convention gathers the biotech ecosystem. (BIO.) |
| 24-27 June, Philadelphia, US: |
| AACR’s malignant lymphoma meeting puts blood cancers back in the precision medicine spotlight. (AACR.) |
Follow the last-mile conversation!
IPM Alliance tracks the decisions, bottlenecks and implementation gaps shaping personalised medicine access. Follow us for briefings, events, policy signals and practical insights from across regions and disease areas.
We want to hear from you
When a patient becomes eligible for personalised care, where does the system most often lose them: identification, testing, referral, reimbursement, delivery capacity or equity?
Know someone who should be reading this?
IPM Brief is built for people working where science, policy and patient access collide. If one colleague would find this useful, forward it to them and help bring them into the conversation.
International Alliance for Personalised Medicine
Avenue de l’Armée / Legerlaan 10, 1041 Brussels, Belgium
This email was sent to jayasinghtec29@gmail.com. You are receiving this email because you are part of the IPM Alliance network or have engaged with our activities, briefings, events, or policy work.
{kind=link}